

Behavior Training Series
This video-based series is available to help explore the possible root causes of challenging and aggressive behaviors and identify possible solutions.
Modules in the Series
Select from the list below to see details about the module and begin.
This module will:
Help you understand how challenging behaviors may develop
Give an overview of what a Functional Behavior Assessment is and how to conduct one
Use the Functional Behavior Assessment to identify events that trigger or set off the challenging behavior and the reasons it may continue to occur
To begin
Click the titles of the sections below to expand and complete each section.
A transcript of the module is available. Use it to read instead of watch the videos or to follow along.
1: Aggression in typically developing children and how it may develop in Individuals with AS
2: Forms of Aggressive Behavior in Individuals with AS
Aggressive behavior in individuals with Angelman syndrome can be separated into two categories:
1. Physical aggression toward people
- Hitting
- Kicking
- Scratching
- Pinching
- Biting
- Hair pulling
- Grabbing
Sometimes, an acceptable behavior can turn into an aggressive behavior. For instance, hugging someone can turn into hair pulling or grabbing.
2. Aggression toward the environment:
- Throwing or breaking objects
- Ripping, shredding or pulling apart objects
3. Prevalence of Aggressive Behavior in Individuals with AS
Challenging behavior such as aggression has been reported in less than 10% to as many as 100% of individuals with AS. A major reason for this variability is different methods have been used to study aggressive behavior.
Reviews of case studies in the published literature have yielded low estimates, since many of these studies focus on the genetic rather than behavioral aspects of AS. Studies that are designed to look at behavioral issues tend to provide higher estimates, perhaps because many of the parents and caregivers who choose to participate in these studies are motivated to do so because they are already concerned about challenging behavior. More information is needed about the “true” prevalence of aggressive behavior in individuals with AS. Information is also needed about different aspects of aggressive behavior (what types of aggression occur, whether it improves or gets worse over time) as well as the impact of different interventions (behavioral approaches, medication) on aggressive behavior.
4: Genetics of AS and Risk Factors for Aggressive Behavior
Certain factors are known to place individuals with intellectual disabilities (including those with AS) at risk for developing challenging behavior, including aggressive behavior.
- Being nonverbal
- Having mobility problems
- Having severe cognitive impairment
- Having seizure disorder
Many of these risk factors are in fact primary characteristics of AS.
There is no evidence of a direct link between the genetic defect that causes AS (UBE3A deficiency) and aggressive behavior. There is also no evidence that aggressive behavior is related to an individual’s specific genotype (deletion positive, gene mutation, uniparental paternal disomy or imprinting center defect). However, UBE3A deficiency does result in conditions, impairments and specific behavioral features that may increase the risk for individuals with AS to develop aggressive behavior. Furthermore, since behavior occurs within a broader context, social and environmental factors can modify (increase or decrease) the expression of aggression and the impact that it has on the individual’s life. Rather than being caused by one or the other, it is likely that both biological and environmental factors interact to influence how aggressive behavior develops and continues in individuals with AS.
At the present time, we can’t change the genetic defect that causes AS. However, we can try to decrease the risk that aggressive behavior will develop and continue over time by the following. First, we can try to reduce the impact of underlying conditions and impairments that can lead to behavior problems by optimizing the individual’s physical and emotional health and potential for learning. Second, we can try to replace aggressive behavior with new skills that will increase the individual’s personal and social competence, so that aggression is no longer “necessary.” Third, we can try to remove the inadvertent rewards or “pay off” for aggressive behavior to stop it from occurring and provide rewards for appropriate behavior instead. More complete information about these issues is provided in other modules.
5: Making Sense of Aggressive Behavior in Individuals with AS
Functional Behavior Assessment
Now that you understand aggression a little bit more, here is an introduction to completing a Functional Behavior Assessment followed by step-by-step instructions.
Functional assessment is a process that leads to a better understanding of:
- The factors that make the behavior more or less likely to occur (“setting events”)
- The circumstances that directly set off the behavior (“antecedents”)
- The events that maintain the behavior (“consequences”)
- The reason (“function”) for the aggressive behavior.
A functional assessment can help to explain why the behavior is occurring. After this is complete, a behavior support plan is needed to outline what to do about the behavior. A behavior support plan specifies in detail what needs to be done to decrease the individual’s aggressive behavior and increase more socially acceptable behavior to take its place.
Step by Step Instructions to Complete a Functional Assessment
1: Select and Define the Problem Behavior
The starting point for doing a behavior assessment is to select the problem behavior you want to change and define it in clear, observable terms. This is important in order for everyone to be able to recognize the behavior when it occurs.
Be as specific as possible. Pulling hair, scratching or biting are specific forms of aggression and can be defined more precisely. For example, scratching can be defined as “using fingernails to scrape or dig into someone’s skin.”
In the case of Jack, Jack’s pinching is concerning because he has left bruises on the arms and legs of several of his support workers and pulled their hair very hard, to the point where their scalp is very sore. As a result, they are reluctant to ask him to do many things out of fear that he will hurt them. He is missing opportunities to participate in activities and learn new skills. If the situation does not change, Jack may become isolated from his peers and support staff. Pinching is defined as whenever Jack squeezes someone’s skin between 2 or more fingers. Hair pulling is defined as pulling someone’s hair with one or both hands.
2: Find the Context for Problem Behavior
Once the behavior is defined, it is helpful to survey the social and environmental context in which it possibly occurs.
To help with this, download the Checklist for Identifying the Context for Problem Behavior.
Using the checklist, will help you find answers to questions like these:
- Is the behavior more likely to occur (or less likely to occur) at particular times of the day?
- Is it more or less likely to occur with particular people and in relation to what they are doing at the time?
- Is the behavior more or less likely to occur during particular events, activities or routines?
- Could it be related to how the individual is “feeling” (emotional state, physical health)?
- Are there observable “warning signs” that precede the behavior occurring?
- What happens after the behavior occurs?
- What do you think the individual is trying to “say” through his or her behavior?
Summarize What you Learned about the Context of the Behavior
Summarize your findings using the Summary of Contextual Information form.
See Completed Examples of Jack’s Assessment
See an example of a completed checklist of contextual factors.
See an example of a completed summary.
Based on the responses of Jack’s support workers, Jack’s aggression is more likely to occur:
- when he is ill, hungry, tired or in an angry/bad mood
- when he is with two particular support staff as well as unfamiliar support staff
- when he is at the day program, particularly in the morning
- when he is being changed, has to wait for meals or walk long distances
- when support workers are paying attention to someone else, tell him to do something he dislikes or tell him that something he likes is not available or is finished
- he is often given what he wants after behaving aggressively or something he doesn’t like is stopped or changed
In addition, he seems to be “saying” he wants something, he doesn’t want to stop what he is doing or he doesn’t want/like something when the aggression occurs.
3: Track the Problem Behavior
At this point, you have selected and defined a problem behavior and have learned more about the context of when the behavior occurs. Now, it’s time to track the problem behavior over several days to a week.
In order to gather valid information, it is necessary to observe the individual in different environments, at various times and with a variety of people.
Track the following about the problem behavior:
- Frequecy: how often the aggressive behavior occurs
- Duration: how long it lasts
- Intensity: how severe it is
Download the Behavior Tracking Sheet.
What you can learn from tracking
Some aggressive behavior such as biting may not occur very often or last very long, but can be severe when it does occur and cause injury to others. Other aggressive behavior such as grabbing at people may occur frequently and last longer in duration, but be milder in intensity.
It is not uncommon for people to make general statements about aggressive behavior – for example “He seems to hit me every time I ask him to do something” or “It seems like she can’t go longer than a day without pinching someone.” Behavioral tracking provides objective, quantifiable information rather than relying on people’s judgment or impressions which may not be accurate. It can be reassuring to learn that aggressive behavior may occur much less frequently than first thought. Returning to the previous examples, “I asked him to do 10 things today and he actually hit me once” or “She pinched her worker only once in the past 2 weeks.”
Paying close attention to frequency, duration and intensity of the problem behavior is an important step and will help sharpen your observational skills. It can also help prepare you to directly record more extensive information about episodes that involve the problem behavior for the next step.
See a completed Example Based on Jack
See Jack’s completed tracking form.
Jack’s support workers have tracked his aggressive behavior (pinching others and pulling hair) over a one-week period. Since they are all busy attending to the individuals in the day and residential programs, they shared the responsibility for tracking Jack’s behavior by setting up a schedule that assigned specific staff to cover specific periods of time (for instance, Support Worker A tracked Jack’s behavior from 9 – 11 am, Support Worker B from 11 am – 1 pm, and so on).
4. Collect A-B-C Data
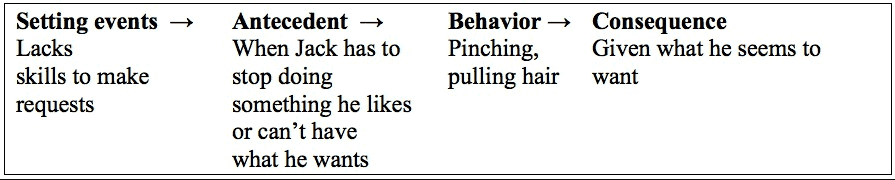
Jack’s support workers have been given an A-B-C chart to help them keep a detailed record of his pinching and hair pulling. Since their “roster” system worked so well for tracking when Jack’s behavior occurred, they decided to use this approach when recording behavioral episodes. The table to the right shows how this information is recorded on an A-B-C chart. Jack’s support workers record what happens immediately before he pinches them or pulls their hair (“antecedents”) as well as what they do in response to the aggression (“consequences”).
The immediate antecedent (“trigger”) for pinching was when the support worker said “Come, let’s go put the toy back” and tried to guide Jack out of the chair. The support worker responded to being pinched by yelling and backing away from Jack; she also left him alone on the chair (“consequence”).
The worker had been sitting at the table with Jack, assisting him to do a puzzle. He walked away from the table and went to sit in his favorite chair. The worker tried to “entice” Jack to get up from his chair and come back to the table by showing him a toy. She asked him numerous times to get up (“Let’s go put this on the table”). He tried to scratch her and reached out to pinch her or push her arm out of the way a number of times but she was able to pull away. He also turned away from her.
After the worker finished recording what had happened, she was asked how Jack’s morning had gone. She said he seemed tired when he arrived at the day program and had gone to sit in his favorite chair. He covered his face with a blanket and went to sleep for an hour. She was able to get him to come to the table to do a puzzle for a couple of minutes rather than let him sleep all morning in the chair.
5: Link the Aggression to Antecedents and Consequenses
It is not possible to identify the function of a behavior based on information from only one incident. Information needs to be collected over a longer period of time (perhaps several days) in order to get a more thorough picture of the individual’s aggressive behavior and the circumstances that surround it. Once A-B-C information has been gathered, it can be reviewed to identify patterns and generate ideas (“hypotheses”) about the function of the aggressive behavior.
People may have a variety of opinions about why the aggressive behavior occurs, but it is always better to collect systematic information to see if their opinions are supported by facts.
Information from the A-B-C form can be used to summarize a behavioral episode.

When the worker was asked her opinion about what was Jack trying to “say” at the time he pinched her,
she thought he was saying “Leave me alone, I want to stay in the chair.” In this situation, the “function”
of Jack’s behavior may have been to continue with a preferred activity (sitting in the chair).
6: Tie Your Findings Together
Once Jack’s support workers finished with the functional assessment, they tried to summarize the information they had gathered. They observed 10 episodes (or instances) of pinching and hair pulling during a one-week observation period. On 6 occasions (60% of the time), the behavior was preceded by a support worker stopping something that Jack enjoyed. On 2 other occasions (20% of the time), the behavior was preceded by a support worker telling Jack he couldn’t have something he wanted. All together, there was an 80% chance that Jack would pinch support workers or pull their hair if his access to a preferred item or activity was restricted or prevented. On 7 occasions (70% of the time), the behavior resulted in Jack being given something he liked or being permitted to continue what he was doing. Based on the outcome of the functional assessment, the function of Jack’s aggression (pinching and hair pulling) was hypothesized to gain or maintain access to something he wanted.
With this information in hand, Jack’s support staff were to develop the summary statement.
This module will:
- Understand how AAC can serve as a replacement for aggressive and challenging behavior.
- Recognize the varied nature of communication and language skills across the population of individuals with Angelman syndrome.
- Become familiar with AAC so that you can compare and contrast concepts of effectiveness, efficiency, and naturalness and how these principles relate to developing alternatives to challenging behavior.
- Recognize and provide examples of the four basic components of an AAC system: symbols, strategies, techniques and methods or devices by which communication is conveyed.
- Be able to discuss strategies that can be used to foster individuals’ uses of AAC systems in place of challenging behaviors.
To begin
Click the titles of the sections below to expand and complete each section.
A transcript of the module is available. Use it to read instead of watch the videos or to follow along.
1: Introduction
2: The Relationship Between Behavior and Communication
3. Communication & Language Skills with Case Examples
4: Communicative Intent
5. AS and Communication and AAC
6. AAC Methods and Why AAC is Important
7. How do I know if my individual is a candidate for AAC?
8. Enhanced Natural Gestures
9. Contexts for Effective Communication
10. AAC Systems Efficiency & Naturalness
11. Four Components of AAC
12. Alternatives to Aggression
13. Integrated Objectives
Resources for Communication
- So Much to Say by Dr. Stephen Calculator
- Join the ASF Communication Training Series Facebook group for additional support and tips.
Module Author:
Sarika Peters, PhD
This module will:
- How to select cognitive tasks that are most appropriate for your individual with Angelman syndrome
- How to decrease or minimize aggressive behaviors in situations where cognitive demands may be high.
- How to sort through whether or not your individual with Angelman syndrome has a lot of sensory seeking behaviors and sensory aversions and what you can do to treat or minimize those behaviors.
To begin
- Click the titles of the sections below to expand and complete each section.
- A transcript of the module is available. Use it to read instead of watch the videos or to follow along.
1. Introduction to this module
2. Cognition, Social Cognition and Adaptive Behavior Defined
What is cognition?
Cognition or cognitive development refers to mental processes that include language, memory, attention, pattern recognition, perception, motor skills, and problem-solving. A person may have strengths and/or weaknesses across various aspects of cognition/processes such that they may excel in one domain but have considerable difficulty in another.
The motor aspects of cognition involves mental processing in which the motor system draws on stored information to plan and produce actions, as well as to anticipate, predict, and interpret the actions of others. This involves motor planning, and execution of actions. Cognitive processes are integrated into most of what we do on a daily basis and form the basis for learning/acquiring skills. Social cognition extends these processes to social interactions and involves understanding another person’s perspective/thoughts/feelings, and social norms.
What is adaptive behavior?
Cognition can also influence “adaptive behavior.” Adaptive behavior refers to independent performance of activities of daily living. This refers to broad-based skills (e.g. feeding, dressing, talking, reading, sharing, understanding feelings and emotions, coloring, walking) that must be acquired through development in order to function in and access a variety of settings.
Various aspects of cognition and adaptive behavior are often measured for children/adults to receive special services. These evaluations are typically conducted individually by a psychologist. Teachers and parents typically act as informants for adaptive behavior. Taken together, an evaluation of cognition and adaptive behavior provides an estimate of an individual’s level of understanding/performance and how they may function in school/work settings.
3. Cognitive Processes in Angelman Syndrome
Research has consistently demonstrated that individuals with AS have difficulties with all aspects of cognition. Our experience is that individuals with AS perform better on cognitive tasks that are less abstract, and that involve minimal use of language. Many individuals have difficulties with the motor aspects of cognition, and it may take them longer to demonstrate a skill. Depending upon the nature of the cognitive task and how demanding it may be, individuals with AS may exhibit aggressive and/or challenging behaviors. These may include throwing objects, mouthing objects, hitting others, spitting, pinching, kicking, biting, hair pulling, and/or attempts to leave the room/run. We have also experienced/observed tight hugs, flopping on the floor, and having an individual put their head down on the table when presented with harder tasks. These behaviors may serve to avoid the difficult task, and/or convey frustration. We have also found that an increase in challenging behaviors may occur as individuals begin to master new skills (i.e. as their cognitive abilities improve), and when they are with a new therapist/teacher.
How to decrease these challenging behaviors
4. Sensory Issues and how they Impact Behaviors
What are sensations?
“Sensations” involve the sight, feel, taste, sound, and smell of things. In order to function effectively, we integrate the information we receive from our senses. This information is then sent to the brain and then it can be acted upon.
When sensory functions are working correctly, they keep us from touching things we should not touch, and eating things we should not eat for example. Disruptions to these processes can result in being hyper-responsive (i.e. over-responsive) to sensory input, or in being hypo-responsive (under-responsive) to sensory input. These disruptions can also result in challenging behaviors across a variety of situations, including situations where cognitive demands are high.
What is hyper-responsiveness?
Hyper-responsiveness – When a person is over-responsive to sensory inputs, they tend to overreact to one or all of the sensory inputs (e.g. touch, smell, movement, vision, hearing, taste, and body position). This is also termed “sensory aversions.” If a person is sensitive to touch, they may dislike the feel of certain types of clothing, not want to wear shoes, be sensitive to lights, and/or dislike the feel/temperature of certain foods. They may also have a very difficult time with medical and/or dental procedures, having their hair brushed or cut, and having their teeth brushed.
Some individuals with sensory aversions may hit others who get too close to them, may throw objects that they do not like the “feel” or taste of, and may scream/yell, and/or cover their ears when overwhelmed by sensory inputs. As applied to classroom based situations, individuals who are over-responsive to touch may not respond well to “hand-over-hand” physical prompts to teach them new tasks. It may take certain individuals some time to calm down after being on “sensory overload.”
What is hypo-responsiveness?
Hypo-responsiveness – When a person is under-responsive to sensory inputs, they may seek out stimulation by mouthing/biting objects, seek out deep pressure by giving tight hugs and/or engaging in more physical play with others, seek movement (e.g. spinning), and it may seem as though they have trouble hearing. They may, for example, hit another person to get them to play and/or greet them. These behaviors can also be called “sensory-seeking” behaviors.
Individuals who are hypo-responsive may not respond to pain/differences in temperature, and they may be highly attracted to lights/shiny objects and may examine things from close visual range (e.g. putting their nose/face right up to the television screen).
5. Sensory Issues in Angelman Syndrome
6. Autism and Spectrum Disorders
Autism – Autism spectrum disorders (ASD) are complex disorders that likely result from a variety of complex combinations of genetic and environmental factors. ASD is characterized by deficits in social affect accompanied by restricted and repetitive/stereotyped behaviors.
How is autism diagnosed?
It is a behavioral diagnosis that is made based on direct observations of an individual’s behaviors. There is currently no blood test or medical test (e.g. X-Ray, MRI) that determines whether or not an individual has autism. Physicians may order genetic testing to look for a genetic cause, and they may recommend other tests or studies to determine if other medical conditions are present (e.g. seizures). Often, behavioral observations are done through a formal evaluation with a psychologist. Information about behaviors is also gathered from parents, teachers, and/or therapists in addition to direct observation in order to make a formal “diagnosis” of autism.
What is social affect?
Social affect refers to the appropriate use of eye gaze to regulate social interactions, using a facial expressions, shared enjoyment in interactions, use of nonverbal gestures, and the quality of a social approach. For example, an individual may approach someone else to obtain an object, but not look directly at them, instead being focused primarily on the object of interest. They may hit the other person in greeting, may not use any facial expressions or nonverbal gestures (e.g. pointing, signing), or may even use their hand as a tool to pull the object toward them. Even though this individual approached another person, they clearly have deficits in their social affect skills since the “quality” of this interaction is impaired.
What are repetitive/stereotyped behaviors?
Repetitive/stereotyped behaviors may include hand-flapping, finger-flicking, lining up of objects, and/or spinning of objects. The term “restricted interests” refers to a strong, narrow interest in certain toys or topics (e.g. trains, dinosaurs, birds, cars, plastic bottles) that impair the quality of social interactions with others. An individual may seem “obsessed” with these toys/topics and may have a difficult time with making a transition when these objects are taken away. During times of transition, they may exhibit challenging behaviors. There may be varying degrees of impairments in social affect and restricted/repetitive behaviors, and thus there are varying degrees of “autism.”
7. Autism in Angelman Syndrome
8. Case Study: Bethany
Bethany is a 6-year-old girl with Angelman syndrome (deletion positive). She lives with both of her parents and her typically developing sister. Over the past year, her parents noted that she has made several improvements with regard to her attention span, and her ability to sit still. She also seems to understand more. She has also started to become more independent with her toileting. She currently receives speech therapy school support services, where they are working on using pictures. She receives occupational therapy twice per week, and also receives physical therapy. She uses a friend’s iPad and may use an iPad at school, although this is not always integrated throughout her day. In spite of these clear improvements in cognition, language, and adaptive behavior skills, her parents have become increasingly concerned about her hitting and pinching behavior both at home and at school. This behavior has worsened significantly in the last few weeks. Her parents are unsure of whether changes to her medication regimen could be contributing to these behavioral difficulties. Due to her exhibiting these behaviors in school, they will have a behavior consultant attend the classroom and track her behaviors. In general, she gets along with her peers. She becomes anxious when in medical settings. Recently, a family member was hospitalized and she became very upset when seeing this individual in his hospital bed.
On formal evaluation, she walked with her parents toward the evaluation room but became very anxious upon seeing the room and examiners. She clung to her parents and vocalized. Upon entering the room, she sat on her mother’s lap. She warmed up when shown an iPhone application that played music, though at times she covered her ears (seeming sensitive to the sensory inputs). She made good eye gaze, coordinated with vocalizations and facial expressions to display her like or dislike of the music. It was quite clear that she does not have autism. She was able to transition to testing at the table though needed her mother to sit next to her. She showed good attention for tasks that were easy for her. However, once tasks became difficult, she threw the test materials or hit the examiners. She vocalized and reached for her mother to try to avoid testing. She was responsive to “If-Then” statements paired with visual cues (real objects), re-direction, ignoring of inappropriate behaviors, and some use of visual cues when paired with verbal prompts. She was somewhat tactile defensive when she was upset, and did not like the use of hand-over-hand physical prompts. She frequently gave objects to her mother or the examiner when she was done with them. She mouthed several objects during the assessment. She flapped her arms when excited.
In addition to some of the strategies that have been discussed throughout this module, we recommended that the child’s parents/teachers/therapists work to track her behaviors within the context of any changes to her medications. Specifically, we suggested the use of a functional behavioral analysis, with careful attention to when her behaviors seem to be better and what is occurring during that time. Within the context of the evaluation, her behaviors were quite manageable when she was being presented with tasks that were within her developmental level, but she exhibited several challenging behaviors as tasks became harder. Once the more detailed information has been gathered, we suggested that her parents share this information with the physicians who are monitoring her medications so that any necessary adjustments can be made as needed. They should also monitor any medical issues within the context of significant changes to her behavior.
9. Conclusion
There are situations in which we do believe that an additional diagnosis of autism is warranted along with Angelman syndrome. This will be the case as I said, in a smaller percentage of individuals with Angelman syndrome, but when a diagnosis is warranted, without question we do recommend formal applied behavior analysis as a form of treatment, so that your individual with Angelman syndrome is actually able to fulfill their maximal potential and demonstrate the broad range of skills they do have.
Module Author:
Logan Wink, MD
This module will:
- Techniques to identify mental illness in Angelman syndrome.
- How to prepare for a mental health assessment.
- Identify when it is time to consider treatment with psychotropic medications.
- Become familiar with psychotropic medications and their role in treatment of behavioral concerns in Angelman syndrome.
To begin
- Click the titles of the sections below to expand and complete each section.
- A transcript of the module is available. Use it to read instead of watch the videos or to follow along.
1. Introduction to Mental Illness in Angelman Syndrome
2. Assessment for Suspected Mental Illness in Angelman Syndrome
3. Psychotropic Medication Use in Angelman Syndrome
4. Treatment of Severe Aggressive Behaviors in Angelman Syndrome
5. Case Study: Cate
“Cate” is a 25-year-old individual with Angelman syndrome (deletion positive). Cate lives at home with her mother and father. She suffers from a seizure disorder, requires use of wheelchair to walk long distances, and has a history of bowel and bladder incontinence. Cate does not use a formal communication system, but is able to communicate with some idiosyncratic signs. She also points and leads others to what she wants. She is able to use several word approximations consistently. Cate attends a day program on weekdays, riding the bus to and from her program. In the evenings and on weekends she is home with her parents with no support staff.
Cate has always struggled with impulsivity, especially in social settings. She often will grab at others, pulling at their hair and clothes. Cate also often bangs on the walls of her home to get her parents attention and to get some of her needs met (such as turning on the television or obtaining a favorite food). These behaviors were manageable by redirection when she was younger, however now as an adult they have become more disruptive. Cate often grabs at people in public, limiting her mother’s comfort with taking her out of the home. She also has become disruptive on the bus to day program, grabbing at her aide and at times becoming aggressive while she is strapped in her seat on the bus. Cate’s banging behaviors have also become more troublesome to her parents, as she will bang on the wall between their bedrooms at night when she is awake in an attempt to get their attention.
Cate and her mother worked with a behavioral therapist for several months targeting her “banging” and “grabbing” behaviors. Some improvement in the banging was made through practical interventions such as padding the wall. However the impulsive grabbing continued, and Cate was at risk of not being allowed on the bus to her day program.
At this time, Cate was seen for a psychotropic medication evaluation. Following a great deal of discussion, the decision was made to start Cate on a low dose of Seroquel (quetiapine) targeting her impulsive and irritable behaviors. At the initial dose of Seroquel, little changed with Cate’s behavior. However, as the medication was slowly increased to three times per day dosing, Cate’s behavior began to improve. There was a notable reduction in her behavior on the bus, much to the relief of her aide and the bus driver. Cate was more easily redirectable away from her banging behaviors. She also began to sleep a bit better at night. Unfortunately Cate did experience some sedation with this medication, which limited increasing the dose further. However, over time she was able to tolerate a dose that was helpful with her behavior without being overly sedating.
6. Conclusion
Individuals with Angelman syndrome are at risk of the development of mental illness, just like those of us without developmental disabilities. When severe changes in behavior, mood or functioning occur, mental illness should be considered as a potential cause. In those cases, individuals should be evaluated by a certified mental health practitioner such as a psychologist or a psychiatrist. When mental illness is identified, often there are medications that can be used to help treat these symptoms. Medications for anxiety and depression are often quite effective, and in the rare cases of severe disruptive or aggressive behavior, atypical antipsychotics can often help with these behaviors.
Module Author:
Ron Thibert, DO
Pediatric Epilepsy Specialist and Director of the Angelman Syndrome Clinic at Massachusetts General Hospital in Boston, MA
This module will:
- Understand how an increase in seizure activity might result in an increase OR decrease in aggression.
- Describe the typical patterns of sleep problems in AS and management strategies.
- Describe the common gastrointestinal, orthopedic and mobility issues in AS.
- Understand how unrecognized pain may manifest as a direct or indirect change in behavior.
To begin
- Click the titles of the sections below to expand and complete each section.
- A transcript of the module is available. Use it to read instead of watch the videos or to follow along.
1: Introduction and General Information about seizures in AS
2. Seizure Activity and Tracking
Seizure Activity and Behavior
The bottom line is that seizures have the potential to either exacerbate or suppress difficult behaviors depending on the individual, the seizure type, and the behavior. With an increase in epileptic activity in the brain, seizures can draw out more aggressive, hyperactive, and/or defiant behaviors. Our clinical experience has led us to believe that these changes may be related to discomfort, frustration, confusion, or fatigue in the setting of the seizures.
Conversely, we have also seen many children with AS in whom a decrease in seizure activity parallels an increase in difficult behaviors. This type of change is more common when the baseline seizure activity is quite severe, with epileptic activity occurring almost continuously throughout the day and/or night. This kind of persistent epileptic activity can create a sort of barrier between the individual and the outside world, and ultimately have a sedating effect. When this type of severe and persistent aberrant brain activity is suppressed with anticonvulsant medications or dietary therapy, challenging behaviors may in fact increase due to a heightened sensitivity and awareness of the outside world.
One way to think about this is to imagine wearing earplugs, dark sunglasses, and mittens for six months straight. Over time, your brain would acclimate to this decreased level of awareness and sensory input. Seizure activity can act like those earplugs, sunglasses, and mittens, blocking out some of the noise and intensity of the outside world. Then imagine the doctor finds the right medication or combination of treatments to quiet the seizure activity. With this change, suddenly the earplugs come out and the sunglasses and mittens come off. The brain now can perceive and process information from the outside world to a much greater degree. For the individual, this kind of change may feel overwhelming or frightening, and parents and caregivers may see a corresponding increase in aggressive, hyperactive, or defiant behaviors.
Tracking Seizures
To further understand the relationship between an individual’s behavior and his or her seizure activity, it may be important to learn more about the timing and frequency of both the epileptic events and the episodes of challenging behavior. To help determine if seizure activity may be exacerbating an individual’s behavior, it is often helpful to gather data about when seizures are occurring during the day and/or night, and how the events relate to behavioral outbursts.
Example: John’s caregiver kept a log of both his seizure activity as well as his aggressive behavior over several weeks. Four mornings a week, just before breakfast John had a brief seizure. Over the course of two months, on average, at least three out of four of those mornings, less than two hours after the seizure John had a meltdown or displayed aggression towards his aide. In this case, the seizures themselves, or possibly how John felt after a seizure (his ‘post ictal’ state) may have been driving the behavioral outbreaks.
The more data we can gather about seizure timing and frequency, the more equipped you and your doctor will be to make informed treatment decisions, so as to optimize seizure control and potentially improve behavior.
www.seizuretracker.com is a helpful website for logging seizures over time.
3: Epilepsy Management Strategies
Seizures in AS can be quite challenging to treat, but it is very important for clinicians and parents to relentlessly pursue seizure control, because with time and sometimes multiple treatment trials, the majority of individuals will achieve a reduction in seizure frequency.
Individuals with AS, in most cases, should be routinely followed by a neurologist and/or epilepsy specialist who can work to optimize treatments as well as monitor for medication side effects and toxicities. Levetiracetam (Keppra), lamotrigine (Lamictal), and clobazam (Onfi) are three antiepileptic medications that we commonly use to treat epilepsy in the AS population; however, every person is different and treatments must always be uniquely tailored to the individual.
Additionally, we have had wonderful success with the treatment of AS-related seizures using dietary therapy. Specifically, high fat, low carbohydrate treatments, including the ketogenic diet and the low glycemic index treatment (LGIT), have proven effective in AS. For more information about diets, go to Resources.
4. Antiepileptic medications
5. Sleep
Common sleep issues
Difficulties may include:
- trouble falling asleep
- reduced total sleep time
- frequent night wakings
- irregular sleep-wake cycles
Fortunately, sleep problems tend to improve with age.
Sleep Improvement Strategies
There are many sleep treatment strategies to try to improve sleep:
- improving an individual’s sleep hygiene
- external sleep factors like bedtime routines
- minimization of distractions in the sleep environment (sound, light, toys)
- an increased exercise, and/or dietary modifications such as limiting sugar intake can improve sleep
- medications have proven very helpful for sleep (discuss melatonin and gabapentin (Neurontin) with your neurologist)
6. Orthopedic health and mobility
7. Gastrointestinal health
8. Identification and management of pain
Frequently Asked Questions
Q: Why is it important to track behavior?
It is important to track behavior in order to obtain accurate information about what is happening, rather than relying on people’s subjective impressions. By tracking behavior over time, it is possible to determine whether your support plan is successful.
Q: Why is it important to do a functional assessment?
Research has shown that behavior support plans are more likely to be successful if they are based on the results of a functional assessment.
Q: How long should I track behavior? How much information do I need to gather?
There is no set answer to this question. It is necessary to obtain enough information over a sufficiently long period of time to be able to identify patterns in the individual’s behavior. If the behavior happens frequently, in many situations with many different people, it may be possible to get a good sample relatively quickly. If the behavior occurs less often or is very unpredictable, it may take longer to get a good sample.
This project was funded by the Canadian Angelman Syndrome Society (CASS) and the Angelman Syndrome Foundation (ASF), and developed by the ASF.
“Jack” is a 27-year-old individual with Angelman syndrome (deletion positive). Six months ago, he moved from a group home where he had lived for 8 years to a new group home and day program. Staff at the new agency did not receive much information from his previous placement to help with his transition. They were told he is taking risperdal because of challenging behavior.
Jack has a seizure disorder and is taking 3 different anti-epileptic medications. He has not suffered from any grand mal seizures since moving to the new agency but does have drop seizures several times daily. Jack’s foods are pureed and his liquids need to be thickened due to a history of aspiration. He is able to use a spoon to feed himself but this can take a long time. Jack is able to walk independently but uses a wheelchair when required to walk for longer distances. He wears ankle-foot orthotics and requires assistance on stairs.
Jack does not have a formal communication system and communicates by pointing and leading people to what he wants. He uses idiosyncratic signs, such as leaning toward another person and placing the side of his head or cheek against them to indicate acceptance (“I like you”). He has a single word approximation – “om” for home. He is able to understand routine instructions in context.
Jack has a number of interests, such as watching videos and looking at photos (they need to be laminated to prevent him from ripping them). One of his favorite activities is to sit by a window and watch people walk past outside.
Jack’s support workers used to be able to divert his attention to get him to cooperate but now he is starting to pinch and hit them and pull their hair. This happens during activities of daily living, such as when they try to change him. He may also become aggressive when they try to stop him from getting his coat when he thinks it is time to go home. At these times, he will say “om” and gesture toward the door. He often spends all morning at the day program resting or sleeping, and will cover his head with a blanket and become aggressive toward support workers if they try to get him up for activities. He appears to target a particular female support worker who has a very animated personality
Jack’s support workers want to know how they can decrease his aggressive behavior and improve his communication and leisure skills.